Subcutaneous Dirofilaria
(Dirofilaria repens)
Dirofilaria repens is a filarial nematode of dogs (and cats) transmitted by mosquitoes. The adult worm commonly found in sub-cutaneous tissue deposit microfilariae that circulate in blood. Dirofilaria repens is zoonotic.
| Parasite: Dirofilaria repens* |
| Common name: Subcutaneous Dirofilaria |
| Host: Dogs, wild canids |
| Pre-patent period: 120-180 days |
| Location of adults: Subcutaneous tissue and peri-muscular fasciae |
| Distribution: Africa, southern and central Europe, Asia |
| Transmission route: Mosquitoes |
| Zoonotic: Yes |
* Other Dirofilaria spp. or strains have been reported as causative agents of subcutaneous dirofilariosis in dogs (e.g., “Candidatus Dirofilaria hongkongensis”), but further research is needed to confirm their identity and/or pathogenic role.
Distribution
Dirofilaria repens has been reported in Africa, the Middle East, Europe and Asia.
Clinical signs
Infection may be asymptomatic or most commonly present as generalised dermatological lesions as a result of a hypersensitivity reaction to microfilariae. This includes pruritus, erythema, papule formation and secondary alopecia and excoriations [1]. Subcutaneous nodules harbouring adult worms are occasionally observed.
Diagnosis
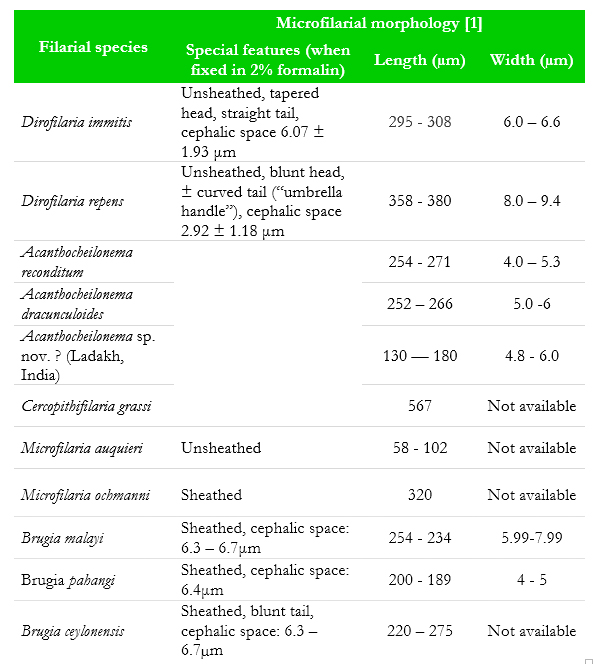
Identification of circulating microfilariae in whole blood using a microfilarial concentration technique (e.g. the modified Knott’s method (SOP 5)) is the diagnostic test of choice. If a nodule is observable, cytological examination of the fine needle aspirate may reveal the presence of microfilaria. Currently, no serological test kits for the detection of D. repens are available. In many geographical locations circulating microfilarial densities peak in the late afternoon and evening, especially once the animal has eaten a meal. Blood collection during these periods will reduce the probability of a false negative microfilarial detection test. Care should also be taken to morphologically differentiate microfilariae of D. repens from other filarial parasites occurring in the area (see Table 3) (e.g. D. immitis, Acanthocheilonema spp., Brugia spp.). Occult infections (lack of observed microfilariae) may complicate diagnosis.
Treatment
Treatment is indicated in all positive cases to eliminate the dog as a source of infection to other animals as well as humans. No adulticide therapy for this parasite is registered. An off-label use of two doses of melarsomine hydrochloride at 2.5 mg/kg IM into the lumbar epaxial musculature, 24 hours apart, combined with a single sub-cutaneous injection of doramectin as a microfilaricidal treatment at 0.4 mg/kg 5 days after the initial adulticide therapy, was shown effective as an adulticidal and microfilaricidal therapy [2]. Alternatively, spot-on products containing moxidectin and selamectin are also efficacious as a microfilaricide and when used for longer periods are also efficacious adulticides when administered at labelled monthly intervals [3,4]. Doxycycline 10 mg/kg PO daily for 30 days combined with a single dose of ivermectin 6 µg/kg PO every 15 days for 6 months is also reported as an effective microfilaricide [5]. When present, surgical removal of nodules may be warranted.
Control
Macrocyclic lactones given at labelled recommendations for the prevention of heartworm are also effective for the prevention of D. repens. In endemic areas, chemoprophylaxis with a macrocyclic lactone should commence as early as possible (6 – 8 weeks of age), according to labelled recommendations. Mosquito control through the use of repellents (e.g. pyrethroids) should be applied to the dog.
Table 3 Summary of filarial species infecting dogs and their distinguishing features
Public health considerations
Dogs act as reservoirs for human infection. In humans, the worms undergo migration through the tissues and may be found within nodular lesions under the skin, eyelids and periorbital tissue, mouth, female breasts and male genitals. These nodules are often confused with neoplasms and eventually may be removed surgically.
References
[1] Talerro W.Clinical aspects of dermatitis associated with Dirofilaria repens in pets: A review of 100 canine and 31 feline cases (1990–2010) and a report of a new clinic case imported from Italy to Dubai. J Parasitol Res. 2011;578385.
[2] Baneth G, Volansky Z, Anug Y, Favia G, Bain O, Goldstein RE, Harrus S. Dirofilaria repens infection in a dog: diagnosis and treatment with melarsomine and doramectin. Vet Parasitol. 2002;105:173-178..
[3] Petry G1, Genchi M, Schmidt H, Schaper R, Lawrenz B, Genchi C. Evaluation of the adulticidal efficacy of imidacloprid 10 %/moxidectin 2.5 % (w/v) spotspot-on (Advocate®, Advantage® Multi) against Dirofilaria repens in experimentally infected dogsdogs. Parasitol Res. 2015;114 Suppl 1:S131-44.
[4] Jacsó O, Fok E, Kiss G, Kökény G, Lang Z: Preliminary findings on the efficacy of selamectin in the treatment of dogs naturally infected with Dirofilaria repens. Acta Vet Hung. 2010;58:405-412.
[5] Giannelli A, Ramos RA, Traversa D, Brianti E, Annoscia G, Bastelli F, Dantas-Torres F, Otranto D. Treatment of Dirofilaria repens microfilariaemia with a combination of doxycycline hyclate and ivermectin. Vet Parasitol. 2013;197:702-704.
