Babesia
(Babesia spp.)
Babesia spp. are tick-transmitted piroplasms that infect erythrocytes and constitute one of the most common and significant diseases to affect dogs living in the tropics. Canine babesiosis in the tropics and subtropics is caused primarily by two species, Babesia vogeli (“large” form) and Babesia gibsoni (“small” form).
| Parasite: B. vogeli, B. gibsoni, Babesia rossi, Babesia vulpes |
| Common name: Babesia |
| Host: Dogs and wild canids |
| Incubation period: 1-6 weeks |
| Location in host: IntraerythrocyticI |
| Distribution: Worldwide |
| Transmission route: Ticks, transplacental, blood transfusion, fighting (B. gibsoni) |
| Zoonotic: No |
Distribution
Babesia vogeli has a worldwide distribution, which may be partly explained by its association with the brown dog tick (Rhipicephalus sanguineus sensu lato). Babesia gibsoni has also been found worldwide, but its distribution in some countries (e.g., Brazil) is much more restricted as compared with B. vogeli. Babesia rossi is confined to sub-Saharan Africa. Babesia vulpes is mainly found in Europe and Asia, but in North America (Mississippi, US).
Clinical signs
In general, Babesia gibsoni is more pathogenic than B. vogeli, although the latter is an important cause of mortality in pups less than 12 weeks old. Pathogenicity is greatly influenced by concurrent infection, especially other diseases that cause anaemia (e.g. hookworm infection). Dogs that survive the initial infection become life-long carriers of the parasite despite appropriate treatment and resolution of the original signs. Recrudescence of intraerythrocytic parasites into the bloodstream and the redevelopment of clinical illness may occur at any time in these dogs following stressful situations, immunosuppressive therapy or concurrent disease.
Per-acute babesiosis is characterised by the rapid onset of collapse owing to hypotensive shock. Pale mucous membranes, rapid heart rate, weak pulse, profound weakness, mental depression, vomiting and seizures (occasionally) may be present. Fever may be present but hypothermia is a more consistent finding.
Dogs with acute babesiosis may have been unwell for a few days with non-specific signs such as anorexia, depression, vomiting and lethargy. Clinical findings include pale mucous membranes, dehydration, icterus and hepatosplenomegaly, petechiaepetechiae and ecchymosis, red, brown or yellow-orange urine (haemoglobinuria), vomiting and diarrhoea.
Chronic babesiosis has also been associated with non-specific signs such as anorexia, weight loss, lymphadenopathy, nasal discharge, bleeding tendencies. It is possible that such cases have concurrent ehrlichiosis or other significant disease, and the signs are unlikely to be caused by babesiosis alone.
Diagnosis
A tentative diagnosis can be made in animals with a history of exposure to ticks and associated clinical signs. The aims of the diagnostic investigation for babesiosis should be to i) identify the Babesia parasite(s); ii) search for other infectious agents (especially Ehrlichia spp.); iii) assess the severity of the anaemia; and iv) assess the patient’s overall health status (especially in per-acute cases). Identification of large and small Babesia parasites is made by microscopic examination of a stained peripheral or capillary blood smear (See Figs 1 and 2). Whole blood may also be subjected to PCR, where commercially available. Serological tests may detect antibodies to either or both B. gibsoni or B. vogeli, depending on their specificity. Serological tests may return false negative results in per-acute or acute primary infection.
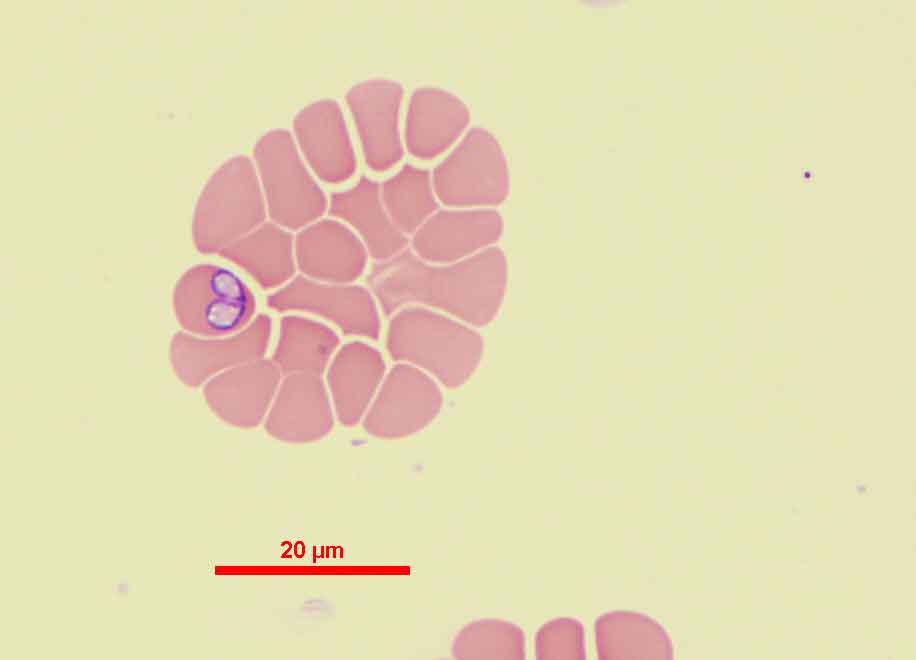
Figure 1 Babesia vogeli within a red blood cell. (Image credit: Dr.P. Irwin)
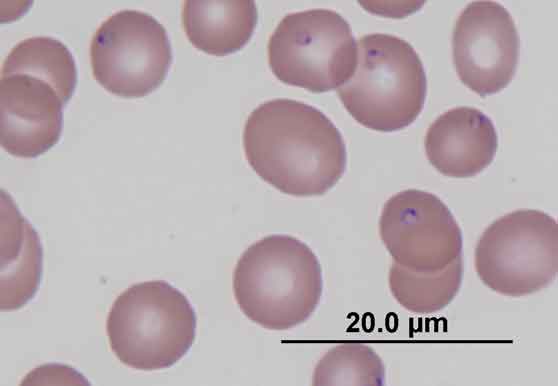
Figure 2 Babesia gibsoni within red blood cells. (Image credit: Dr.P. Irwin)
Treatment
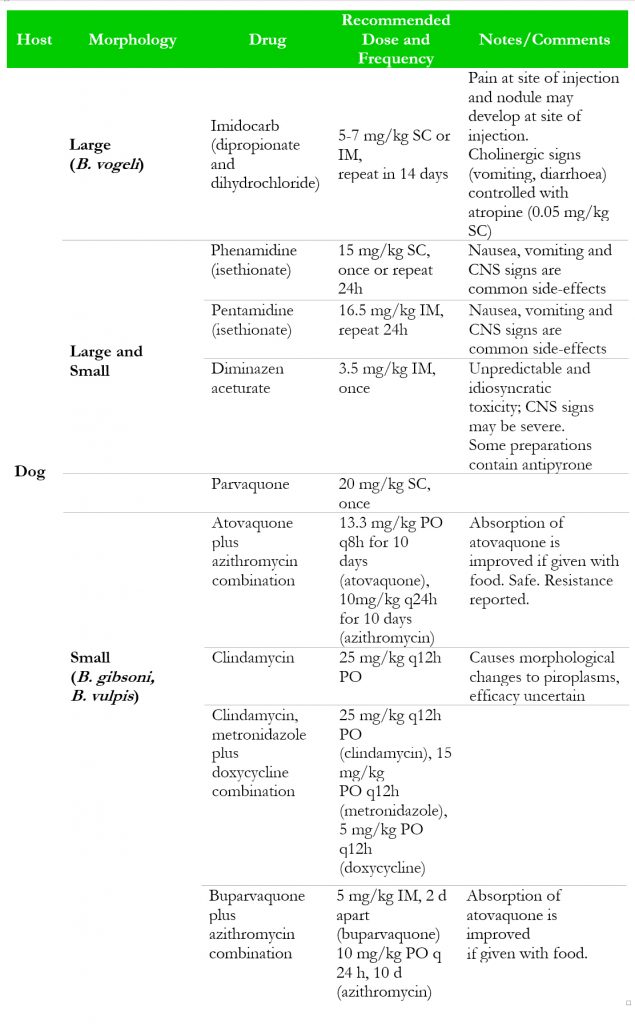
For treatment options refer to Table 2
Many drugs have been used to treat babesiosis, yet very few are consistently reliable. Few, if any, sterilize the infection, and most affected individuals harbour parasites after the treatment is finished. It should be noted that only a few drugs are efficacious against both forms of Babesia.
Blood transfusion in severely anaemic or careful administration of fluids in dehydrated animals may be indicated. Doxycycline at 10mg/kg/day PO (single or divided doses) for 21 days may be used if concurrent ehrlichiosis or other rickettsial diseases are suspected. Glucocorticoids (dexamethasone 0.2 mg/kg IV/SC or prednisolonep 1-2 mg/kg/day divided doses for 5-10 days) have been recommended to ameliorate the immune-mediated haemolysis but the benefit in babesiosis is currently unproven.
The prognosis is variable and difficult to predict in tropical countries. This is probably more a reflection of the effects of concurrent diseases than the Babesia infection. As stated earlier, most dogs become lifelong carriers of Babesia parasites.
Table 2 Dose and efficacy of drugs used to treat babesiosis in dogs. (Click to magnify)
Control
Prevent or reduce exposure to the tick vector by utilisation of registered long-acting acaricides (spot-on/collars) with continuous repel and kill activities (e.g. permethrin, flumethrin, deltamethrin, amitraz), according to labelled instructions. Blood donors should be screened and found free of vector-borne diseases, including Babesia spp. Babesia positive dams should not be bred and dog-fighting disallowed. For further information, refer to tick-control guidelines.
Public health considerations
None.
References
Checa R, Montoya A, Ortega N, González-Fraga JL, Bartolomé A, Gálvez R, Marino V, Miró G. Efficacy, safety and tolerance of imidocarb dipropionate versus atovaquone or buparvaquone plus azithromycin used to treat sick dogs naturally infected with the Babesia microti-like piroplasm. Parasit Vectors. 2017;10:145.