Intenstinal Threadworm
(Strongyloides stercoralis)
Strongyloides spp. infect dogs, cats and humans. Dogs become infected when they ingest infective larvae through mammary milk or when these larvae actively penetrate into the dogs’ skin.
Distribution
Worldwide.
Clinical signs
Most dogs are asymptomatic, developing a strong immunity to infection following transmammary infection and stop shedding larvae within the first 8-12 weeks of life.. In young pups, mild and self-limiting watery or mucus diarrhoea may result. Use of corticosteroids or a reduction in immunocompetence predisposes to autoinfection. In these instances, wasting and signs of bronchopneumonia due to migrationo of auto-infective larvae may be present. Pododermatitis may result from percutaneous penetration of larvae.
Diagnosis
The Baermann technique (SOP 3) is the test of choice for larval isolation and identification. EggsE possess first-stage larvae (Fig 1), which may be isolated on standard faecal flotation (S.G. 1.20) (SOP 1). The first-stage larvae can be recognized via their prominent genital primordium (Fig 2) and must be differentiated from larvae of lungworms (Fig 3) and hookworms. Diagnosis of Strongyloides spp. infection is complicated by the fact that larvae may be very low in number or absent from the faeces, even in symptomatic cases. In these cases, faeces can be tested multiple times (3 times over the course of 5 to 7 ).
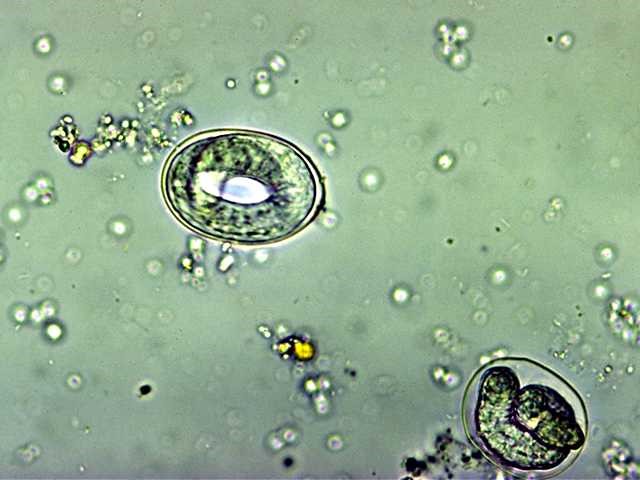
Figure 1 Strongyloides eggs containing first stage larvae on faecal flotation. (Image credit: The University of Melbourne
parasitology image library)

Figure 2 Larva of Strongyloides spp. containing a prominent genital primordium (arrow). (Image credit: The University of
Melbourne parasitology image library)

Figure 3 First-stage larva of a canine lungworm containing a ‘kink’ in the tail. (Image credit: Dr. R. Traub)
Treatment
Off-label use of ivermectin at 200 µg/kg, as a single oral dose and fenbendazole 50 mg/kg once daily for 5 days is effective at removing adult worms. Re-test faeces twice at 2- and 4-weeks following treatment and monthly thereafter, for a total period of 6 months. Re-treatment may be necessary in some cases.
Control
In Strongyloides-endemic areas, consider testing dogs prior to initiating any immunosuppressive therapy, particularly corticosteroids. Latent intestinal infections can be reactivated when the host is immunocompromised (e.g. iatrogenic, neoplasia) to produce auto-infective larvae, which can cause life-threatening disseminated infection. Infected dogs should be isolated from other animals. For further control options, refer to the General Considerations and Recommendations section.
Public health considerations
In humans, clinical signs of S. stercoralis infection may range from being asymptomatic to causing gastrointestinal disorders (e.g. abdominal pain, diarrhoea) and cough. Percutaneous penetration of infective larvae may also cause larva currens. In immunocompromised people, autoinfection may result in hyper-infection syndrome, disseminate strongyloidiasis and bacteraemia, which may prove fatal.